Clinical Toxicology — For Healthcare Organizations
For healthcare organizations and professionals (B2B) · Physician-led · Updated 2026-07-12 · CLIA #45D2048957 · CAP #8722734
LC-MS/MS definitive confirmationCLIA #45D2048957 · CAP #8722734 · Same-day results · Walk-ins welcome
We compete on two things only: turnaround time and testing quality. Not on billing, not on referral incentives, not on anything that would put your compliance officer in a difficult conversation. That is a deliberate position, and it is stated in writing further down this page.
What we run: urine drug testing and oral fluid, with LC-MS/MS definitive confirmation and quantitation, 12–48 hour turnaround, in a CLIA-certified (#45D2048957) and CAP-accredited (#8722734) high-complexity laboratory under an MD laboratory director.
Why definitive testing is not an upsell: an immunoassay screen tells you a drug class, not a compound. It cross-reacts. It produces false positives that damage the patient relationship, and false negatives that hide real risk. When a result is going to change a clinical decision, a class is not an answer.
What we run: urine drug testing and oral fluid, with LC-MS/MS definitive confirmation and quantitation, 12–48 hour turnaround, in a CLIA-certified (#45D2048957) and CAP-accredited (#8722734) high-complexity laboratory under an MD laboratory director.
Why definitive testing is not an upsell: an immunoassay screen tells you a drug class, not a compound. It cross-reacts. It produces false positives that damage the patient relationship, and false negatives that hide real risk. When a result is going to change a clinical decision, a class is not an answer.
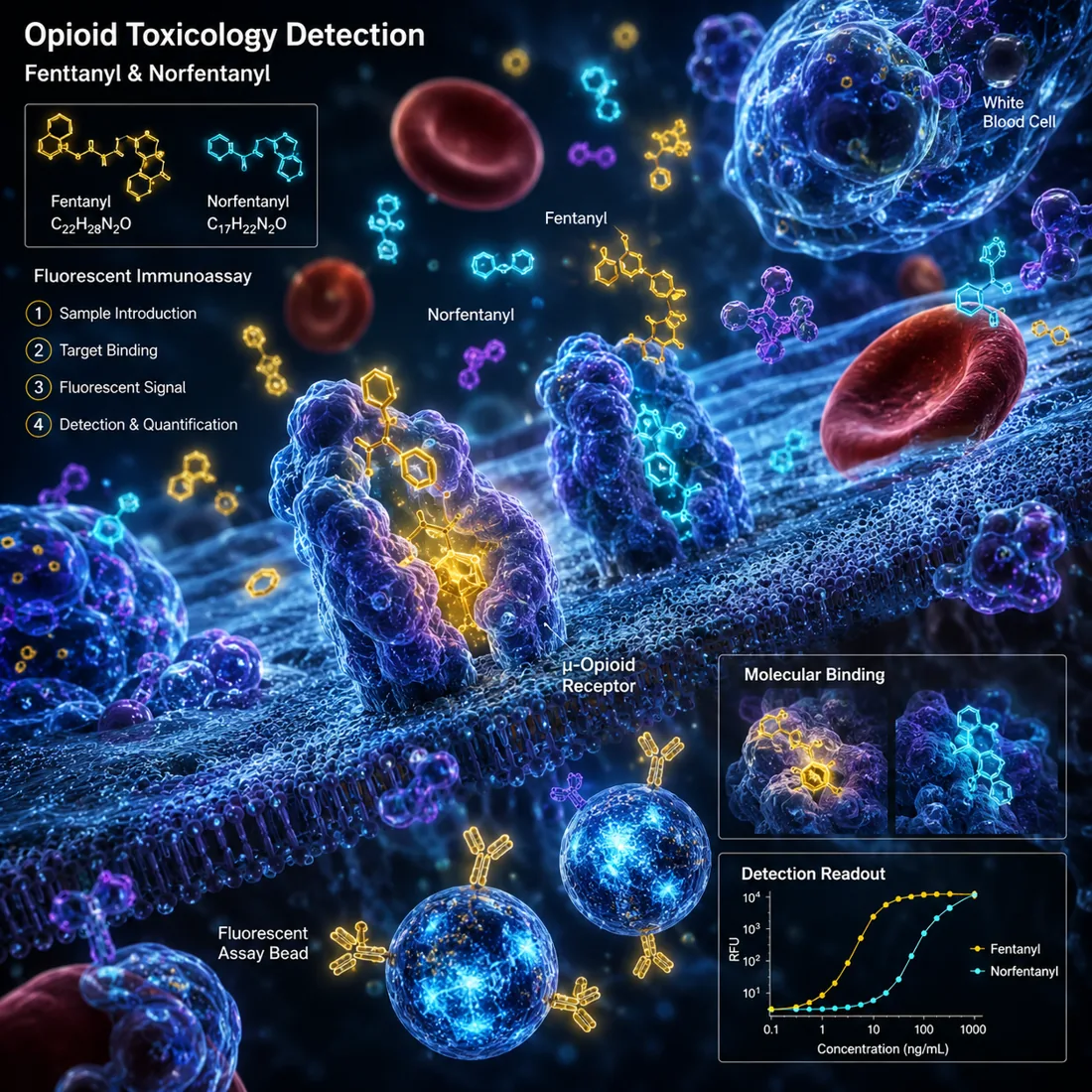
Why this drives the method: fentanyl is potent at very low doses, so the assay has to be sensitive enough to find very little of it. A traditional "opiates" immunoassay is built around the morphine scaffold and largely does not see fentanyl at all.
* Illustrative fluorescence rendering based on the biology and the assay chemistry — not a photomicrograph of a patient sample, and not an instrument output.
New: TB therapeutic drug monitoring. Serum levels for ten anti-tuberculosis drugs by LC-MS/MS — isoniazid, rifampin, rifabutin, pyrazinamide, ethambutol, cycloserine, ethionamide, moxifloxacin, linezolid, pretomanid. See the service →
The blind spot that should worry you most
A negative opiate screen does not rule out fentanyl exposure. Traditional "opiates" immunoassays target the morphine scaffold; fentanyl is structurally different and is largely invisible to them. It requires a dedicated, high-sensitivity method.
The stakes, per CDC: pharmaceutical fentanyl is 50–100× more potent than morphine; roughly 69% of all U.S. drug overdose deaths in 2023 involved synthetic opioids (primarily illicitly made fentanyl), nearly 73,000 deaths — about 22 times the 2013 rate. The fentanyl blind spot, in detail →
The stakes, per CDC: pharmaceutical fentanyl is 50–100× more potent than morphine; roughly 69% of all U.S. drug overdose deaths in 2023 involved synthetic opioids (primarily illicitly made fentanyl), nearly 73,000 deaths — about 22 times the 2013 rate. The fentanyl blind spot, in detail →
What we offer
| Service | Detail |
|---|---|
| LC-MS/MS definitive testing | Specific analyte identification with quantitation; isotopic internal standards |
| Screening vs. confirmation | What each method can and cannot answer |
| Oral fluid vs. urine | Observed collection reduces substitution risk; different detection windows |
| Custom panels | Built around your patient population and clinical question — fewer targets, not more |
| Turnaround | 12–48 hours; TAT = courier + analysis + delivery |
| Quality system | Calibrators, controls, LOD/LOQ, review — the full chain of evidence |
Clinical framework
Testing should answer a clinical question. CDC's opioid prescribing guideline treats toxicology as one tool in risk assessment and monitoring and emphasizes individualization, not blanket protocols. ASAM makes the same point for addiction treatment: a defined clinical purpose, individualized frequency, and results interpreted correctly. The guidelines, summarized →
⚖ Compliance statement (please read). This page is directed at healthcare organizations and professionals. It is not patient advertising. We do not pay for referrals, share revenue, or offer any financial inducement of any kind — in accordance with the Anti-Kickback Statute (AKS) and the Stark Law. All testing must be based on individualized medical necessity determined by the ordering clinician and documented accordingly; we do not endorse blanket or reflex confirmation without individualized justification. Courier, supplies and interfacing services are provided at fair market value (FMV) under written agreement. Our conversations with you will be about turnaround time and testing quality — nothing else. Full compliance page →
FAQ
- Is this a patient-facing service?
- No. Clinical toxicology is offered to healthcare organizations only. Testing must be ordered by a clinician on the basis of individualized medical necessity.
- Why does immunoassay screening need confirmation?
- A screen identifies a drug class, not a compound, and is subject to cross-reactivity. When a result will change a clinical decision, LC-MS/MS identifies the specific analyte with quantitation.
- Will a standard opiate screen detect fentanyl?
- Generally not reliably. Traditional opiate immunoassays target the morphine scaffold; fentanyl requires a dedicated, high-sensitivity method.
- What is your turnaround time?
- 12–48 hours for routine toxicology.
- Do you pay for referrals?
- No. We do not pay for referrals, share revenue, or offer any financial inducement (AKS/Stark). Services are provided at fair market value under written agreement.
- How do we order and receive results?
- Through the Provider Portal, with EMR/LIS interfacing available. Courier pickup can be arranged under written agreement.
References
- CDC — Clinical Practice Guideline for Prescribing Opioids: cdc.gov/overdose-prevention/hcp/clinical-guidance
- CDC — Fentanyl: cdc.gov/overdose-prevention/about/fentanyl
- SAMHSA: samhsa.gov
- ASAM: asam.org
- HHS OIG — Compliance: oig.hhs.gov/compliance
- CMS — CLIA: cms.gov/…/clia
- CAP — Laboratory Accreditation: cap.org/laboratory-improvement/accreditation